Andor Health was born over 4 years ago with a single mission; to fundamentally change the way in which care teams, patients, and families connect and collaborate. By harnessing the latest innovations in OpenAI/GPT models, our cloud-based platform unlocks data stored in source systems - such as electronic medical records - to deliver real-time actionable intelligence to care teams within ubiquitous virtual collaboration platforms like Zoom. By perfecting communication workflows, our platform accelerates time to treatment, decreases clinician burnout, and drives better patient outcomes.
Healthcare institutions and providers use ThinkAndor® to enable providers to configure patient and clinician interactions with ubiquitous team collaboration platforms. This eliminates the need to manage added applications. ThinkAndor® enables a frictionless virtual interaction allowing physicians and patients to communicate without being distracted by disjointed technologies during a virtual consultation.
ThinkAndor is the only integrated virtual collaboration platform that can truly bring together all aspects of outpatient, inpatient, post-acute and at home virtual care collaboration through the 5 Pillars of Virtual Health: Virtual Visits, Virtual Hospital, Virtual Patient Monitoring & Care Management, Virtual Team Collaboration, and Virtual Community Collaboration.
Features include:
- Virtual visits launched from the EHR
- Voice-to-text clinical notes
- Real-time alerts and notifications
- Secure collaboration channels
- ThinkAndor® AI Bot provides relevant content and clinical context to visits and care teams
- Device-agnostic virtual rounding, nursing, sitting and remote consults to power the virtual hospital
- Remote specialty consults such as Tele Stroke, Tele Psych, and Tele ICU
- Access to a virtual on-demand network
- Multi-room/patient virtual sitting for a variety of risk types
- Virtual nursing to address staffing shortages
In 2020, Microsoft M12 took an investment position in Andor Health and works very closely to optimize virtual interactions leveraging OpenAI and GPT. Since then, Andor Health has grown to serve over 70,000 providers and over 500 hospitals leveraging the Andor Health platform across the US, Canada, and UK. Orlando Health, Medical University of South Carolina, Tampa General Hospital, Yale New Haven, and the National Institutes of Health are among some of the most notable. You may find some of our most prestigious partners here, https://andorhealth.com/partners.html.
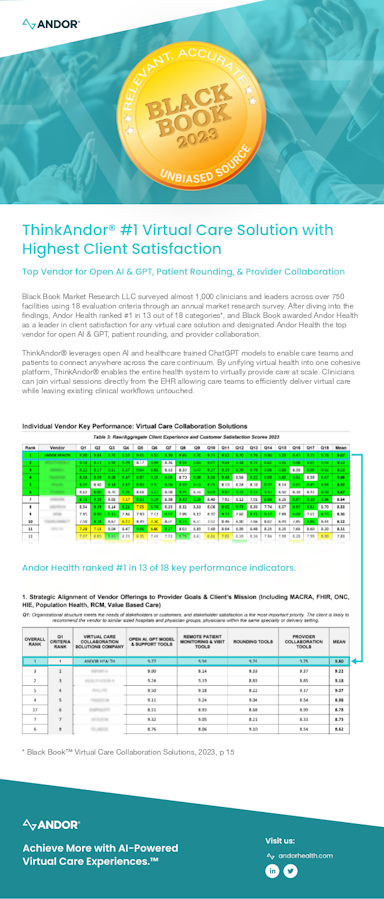
Most Importantly, Black Book has ranked Andor Health as the #1 Virtual Care Collaboration Solution with the Highest Client Satisfaction in 2023! Black Book Market Research used 18 key performance areas of operational excellence to rank Virtual Care Solutions vendors, and recognized Andor Health as the Highest in Client Satisfaction. More importantly, Black Book reached out to nearly 1000 provider organizations, hospitals, and health systems to perform this independent market evaluation with Andor Health taking #1 in 13/18 key performance indicators across all 5 pillars of virtual health & collaboration! This success is a proven indicator of Andor Health’s focus to empower clinicians and care teams with distinct, AI-powered virtual collaboration experiences.